
On Preventing Stroke, TIAs, Clots and Vascular Risk - 30 Years of Experience, and my Dad's Story
On Preventing Stroke, TIAs, Clots and Vascular Risk - 30 Years of Experience, and my Dad's Story
#18 2023 The Rowen Premium Report

Dear Subscriber,
As you may have observed, I have been reporting extensively on what I consider false information on marine oils in the Premium section. The third and final (most important) segment (#17 Part 3) comes out in a few days. If you are taking marine oils, BEWARE. You may be damaging your mitochondria (energy furnaces) as I’ve warned about for many years. In the meantime, I want to answer some really good inquiries I’ve received regarding differences between lumbrokinase (particularly Bolouke) and nattokinase.
I address these here; and, at the end of this report, the Premium subscribers will have my “cocktail” of nutritional supplements, which so far, have been 100% successful in preventing stroke, TIAs, clots (including resolving leg thromboses), etc over many hundreds of patients and nearly 30 years of experience. I hope this information is worth many times your subscription fee for the Premium section. I humbly thank you for subscribing, and ask, if you like the information provided, that you pass on a recommendation to others for these reports. After my experiences with the government over the past year, the Premium section has become a very significant contribution to my sustenance.
I can only speak from our own clinical experience and/or published studies. Actually, I like and place more faith in clinical experience over studies because experience with patients is the real world. Studies might not be at all relevant to any single person.
That said, however, here is a study conducted by the Boluke company comparing their product to nattokinase:
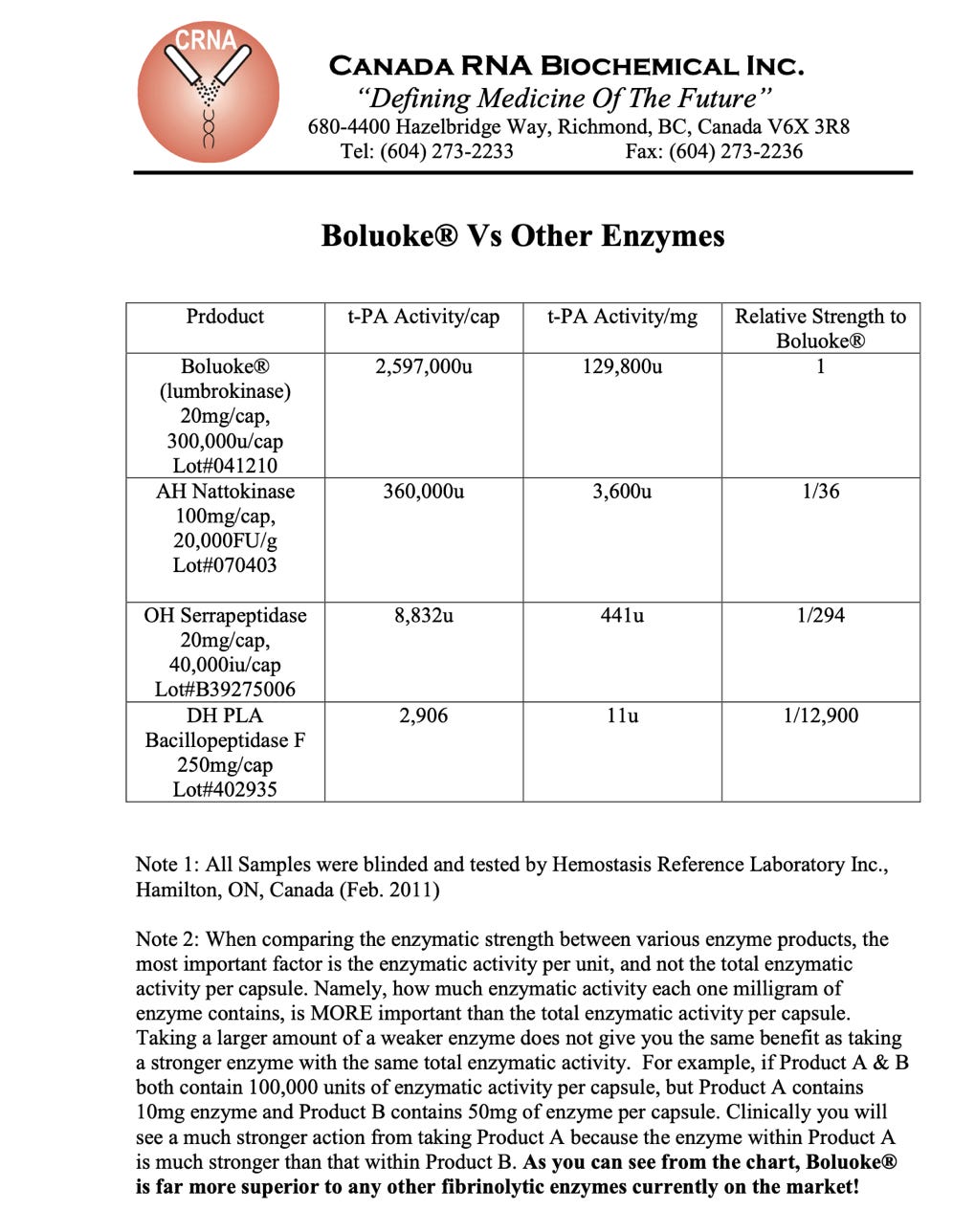
I have to admit, Bolouke version of lumbrokinase looks far superior to nattokinase in ability to dissolve clots. Actually, I accept that. My original mentor on clotting was David Berg, who founded Hemex Lab. We used his lab extensively to measure clotting risk of many of our patients. The key test he had was soluble fibrin monomer. I loved that test for to me, it was a measure of the stickiness of the blood. SFM is like strands of cotton in a cotton ball. The ball is a clot, the strands the SFM. As SFM gets activated, it can form a cotton ball, or a clot. It is these proteins which the kinase enzymes attack and dissolve. David was particularly interested in Lp(a), a protein in blood, which, when high (common) inhibits your ability to break up unwanted clotting. Hence, a huge risk for stroke and clots. Your body has a balance between clotting activity and dissolution of clotting. We need balance in this.
We did scores of tests on patients using his lab. But the raw material for SFM became unavailable (Chinese origin) and my favorite part of the test was lost. He eventually sold off his lab. After so many patients, however, and loss of SFM, I felt I didn’t need to expend patient’s precious funds on the test and treated them empirically based on history and a kinesiology evaluation. We obviously did very well.
Our bodies have two key pathways for clotting. One is platelet aggregation. This pathway is the target of drugs like aspirin, Eloquis, Plavix, etc. If you inhibit platelet aggregation, you will inhibit unwanted clotting, but also raise your risk of not timely clotting when you need to clot. Hence, bleeding with these drugs. Aspirin is well known to induce GI bleeding.
Another Pharma drug is warfarin or coumadin, commonly known as rat poison. This chemical poisons your liver’s ability to make clotting proteins and you will form a clot more slowly. Hence, you are less likely to form an unwanted clot, but far more at risk to bleed since your clotting mechanism will be much slower on the drug. And you will be warned not to eat foods you need, like kale and others which have vitamin K as the mechanism of coumadin is to interfere with vitamin K production of clotting factors in your liver.
There is a far superior way to reduce your risk of unwanted clotting but with little if any risk of raising your chance of bleeding. That is with the enzymes.
Berg preferred lumbrokinase. He was concerned about Lp(a) risk. We measure Lp(a) in all our vascular risk patients. Because of him, we have tended to use Bolouke in cases of elevated Lp(a). Beyond that, I have to admit my choice was how I felt intuitively in the presence of a patient. Perhaps I would use kinesiology to make a determination.
That said, I will tell you of two patients. One, whom we will call “Tom”, a current patient of the office. The other – my dad. First, I’ll add that I have seen at least 350 patients since I first learned of nattokinase in the 1990s. I formulated a cocktail of supplements. Not one of them, to our knowledge has ever had a vascular event, stroke, TIA, bleed, or otherwise.
Then a few weeks ago, I thought our record was broken.
Tom has atrial fibrillation. Years ago, I placed him on my “cocktail” for clotting risk. He faithfully attended the protocol for about 6 years with no event. However, in July 2023, he suffered what was first called a TIA. However, it turns out to be a mild stroke as he was left with very minor cognitive impairment weeks later, though improving, by the time he visited Terri in the office. By definition, a TIA resolves within a few hours or less. I thought our run of good results was broken. However, we discovered that he ran out of Bolouke in December 2022 and did not continue it. He was supposed to take two Bolouke daily. All that time, until he ran out, he was only taking one! And he did so well. Well, now he will be taking at least three daily and will need to do so for life.
My dad had a different story. He was in and out of atrial fibrillation, a huge risk for throwing clots to the brain. And, he had TIAs. He consulted me after his conventional physicians put him on poisons. I objected, telling him we had never seen an event with my cocktail. He presented this to his doctors and they threatened to fire him as a patient if he would not take their poisons. I was living in Alaska and he was in Florida. Too far to be of use for him in case of an event. I did move to California when I married Terri in 2001, but did not interfere with my dad’s program. I’ve learned sometimes it’s best to stay out of family medical matters unless asked.
Dad continued to have TIAs while on the poisons (both coumadin and Plavix, and, I believe aspirin). So, I did recommend my protocol again. And, again his doctors threatened to fire him; and we all knew at nearly 90, he had to have a primary physician. I had reluctance to use nattokinase whilst on the poisons, especially coumadin.
Well, after his conventional doctors violated a black box warning on Lexapro directly on point with my dad’s electrolyte condition, and gave him that poison (for NO good reason other than to push another toxic chemical on an elderly frail man), dad went into a low sodium coma (Black Box warning), and also bled, two months short of his 90th birthday. I flew back to Florida to pay my last respects to him in the hospital and to have it out with his doctors. Mom cooled me. She had spoken to his doctors and they apparently were quite concerned about my anger, knowing that they were fully responsible. They agreed to follow my protocol while he was in the hospital and if he ever got out. I cooled off.
Through a feeding tube they administered my protocol, which in his case involved nattokinase. To the shock of us all, dad awakened 6 weeks later wondering where he was. Mom was great and had visited him in the hospital every day. They were married about 70 years by then.
Dad was transferred to a VA rehab/nursing home center and the doctors continued him on my protocol. Months later, dad left the VA center, first patient I know to have left a nursing home NOT in a casket, after age 90. He lived another 6 years with his beloved (mom) until he fell and had a serious brain injury 2 months shy of 97. He did not die immediately, giving us time to gather. All of his descendants came to Florida and surrounded his bed, including his first grandchild only months old, who sat on his bed. We were sending him love, light and energy. A thunderstorm passed over, and he passed away with all of us around him. It was a very spiritual experience for us all.
The remarkable thing about his case is that in the ensuing 6 years, he did not have a single TIA or vascular event, on my cocktail! This despite the continuing TIAs while taking the Pharma poisons. Mom did not miss a day of giving him the cocktail.
So back to nattokinase and lumbrokinase. As you know, I use Allergy Research Group/Nutricology nattokinase, the company that introduced it in America. I did and still do so because they assay each batch and I want to know that my patients (and dad) was getting what I wanted them to get, especially in a matter where the brain is at risk.
Lumbrokinase is expensive. Each capsule is over $2 apiece. Nattokinase is less than $! Per capsule. A very significant difference in price. Lumbrokinase comes from earthworms. Nattokinase is a vegetarian product, fermented soy extract. I imagine production costs are very different for this reason. So, we have to also consider cost in any equation.
Lumbrokinase is a group of proteolytic enzymes, extracted from Lumbricus rubellus (earthworms). It activates an enzyme called plasmin, which naturally breaks up clots. It is similar in action to a Pharma expensive drug called t-PA for tissue plasminogen activator. Lumbrokinase has not been shown to induce unwanted bleeding. Pharma t-PA is risky.
Nattokinase is known for its ability to induce fibrinolysis (clot dissolution) as well. And I’ve recently presented information on other incredible properties, including lowering of lipids, blood pressure, and plaque thickness in patients in a China study.
So, when it comes to these two wonderful products, I have to go on my intuition. In hundreds of patients, we’ve not had a vascular event, using either. That has to beat Pharma by miles if not light years. Tom was only taking one Bolouke a day and did well. Most of our patients using nattokinase have taken 1 twice daily. Based on the recent China study, up to 5 nattokinase might well be used due to seemingly added benefits beyond preventing clots. While Bolouke may be many times more fibrinolytic than nattokinase, in our hands, we’ve seen no difference clinically, and clinical experience is most important to me. One of my original mentors, Garry Gordon, DO, collaborated with me on risky patients and he saw no cardiac/thrombotic events either in hundreds of his patients. So, we knew well we were on to something terrific.
Getting down to cost. Using 5 nattokinase a day will cost about the same as 2 Bolouke per day. You can get a substantial discount on either product at Allergy Research Group using the code 10-0051. (This code gets you a very substantial discount on ALL their fine products, but you must go through the ARG company itself to use it.) Their lumbrokinase comes from the Bolouke company, so you are getting the real McCoy, and at a discount.
I can’t suggest one or the other in an educational article like this. If it’s clot prevention you need, either/both have worked superbly in our hands. With the latest information on nattokinase, we will want to see what increasing the dose to 5 per day will do for blood pressure and other vascular risks. I would bet that we’ll see little difference between lumbrokinase and nattokinase at these doses. (However, for Lp(a) issues as I have indicated, we do use lumbrokinase. David Berg believed it specifically addresses the biochemical anomaly in this genetic condition). Lp(a), when elevated, suppressed the natural activity of your plasminogen, reducing clot dissolution and substantially raising vascular risk.
So now for my “cocktail”. I decided to approach clot risk issues from several mechanisms, and to our relief, “Tom” did not break our success streak. (He broke the protocol!)